
12.2 Calcium
Calcium
Calcium is a macromineral and the most abundant mineral in the body. The reason for calcium’s
abundance is its distribution in the skeleton, which contains 99% of the calcium in the body. For more information on calcium, see the Required Web Link below.
Required Web LinkCalcium Fact Sheet for Health Professionals
Links
Calcium Fact Sheet for Health Professionals – https://ods.od.nih.gov/factsheets/Calcium- HealthProfessional/
Subsections:
- 12.21 Calcium Absorption
- 12.22 Calcium Bioavailability
- 12.23 Calcium Functions
- 12.24 Calcium Deficiency & Toxicity
Calcium Absorption
Calcium is taken up into the enterocyte through Transient Receptor Potential V6 (TRPV6), a calcium channel found on the brush border. Calbindin is the calcium binding protein that facilitates uptake through TRPV6 and transport across the enterocyte. Ca2+-Mg2+ ATPase functions to pump calcium out of the enterocyte and into circulation and to pump magnesium into the enterocyte, as shown below1.

Figure 12.211 Calcium uptake and absorption
As we have previously discussed, increased calcitriol synthesis in the kidney causes increased binding to the vitamin D receptor, which increases calbindin synthesis. Increased calbindin ultimately increases calcium uptake and absorption.

Figure 12.212 Increased calbindin increases calcium absorption
There are a couple of calcium-binding compounds that inhibit its absorption. Therefore, even though some foods are good sources of calcium, the calcium is not very bioavailable. Oxalate, found in high levels in spinach, rhubarb, sweet potatoes, and dried beans, is the most potent inhibitor of calcium absorption2. Recall that calcium oxalate is one of the compounds that makes up kidney stones. Based on this understanding, it should not be a surprise that formation of this compound inhibits calcium absorption. Another inhibitor of calcium absorption is
phytate. Phytate is found in whole grains and legumes2. So, ironically, the whole grains in your breakfast cereal can actually reduce slightly the amount of calcium you absorb from the milk you put on that same cereal.
References & Links
- Gropper SS, Smith JL, Groff JL. (2008) Advanced nutrition and human metabolism. Belmont, CA: Wadsworth Publishing.
- Shils ME, Shike M, Ross AC, Caballero B, Cousins RJ, editors. (2006) Modern nutrition in health and disease. Baltimore, MD: Lippincott Williams & Wilkins.
Calcium Bioavailability
Calcium bioavailability varies greatly from food to food, as shown in the table below. This table gives the serving size, calcium content of that food, and percent absorbed. The calcium content is multiplied by the absorption percentage to calculate the estimated calcium absorbed. Finally, it shows the servings of each food needed to equal the estimated calcium absorbed from 1 serving of milk.
Table 12.221 Bioavailability of calcium from different foods sources1-3
|
Food |
Serving Size (g) |
Calcium content (mg) |
Absorption (%) |
Estimated Calcium Absorbed |
Servings needed to equal 240 mL milk |
|
Cow’s Milk |
240 |
300 |
32.1 |
96.3 |
1.0 |
|
Almonds, dry roasted |
28 |
80 |
21.2 |
17.0 |
5.7 |
|
Beans, Pinto |
86 |
44.7 |
26.7 |
11.9 |
8.1 |
|
Beans, Red |
172 |
40.5 |
24.4 |
9.9 |
9.7 |
|
Beans, White |
110 |
113 |
21.8 |
24.7 |
3.9 |
|
Bok Choy |
85 |
79 |
53.8 |
42.5 |
2.3 |
|
Broccoli |
71 |
35 |
61.3 |
21.5 |
4.5 |
|
Brussel Sprouts |
78 |
19 |
63.8 |
12.1 |
8.0 |
|
Cabbage, Chinese |
85 |
79 |
53.8 |
42.5 |
2.3 |
|
Cabbage, Green |
75 |
25 |
64.9 |
16.2 |
5.9 |
|
Cauliflower |
62 |
17 |
68.6 |
11.7 |
8.2 |
|
Cheddar Cheese |
42 |
303 |
32.1 |
97.2 |
1.0 |
|
Chinese mustard greens |
85 |
212 |
40.2 |
85.3 |
1.1 |
|
Chinese spinach |
85 |
347 |
8.36 |
29 |
3.3 |
|
Fruit Punch (CCM) |
240 |
300 |
52 |
156 |
0.6 |
|
Kale |
85 |
61 |
49.3 |
30.1 |
3.2 |
|
Kohlrabi |
82 |
20 |
67.0 |
13.4 |
7.2 |
|
Mustard Greens |
72 |
64 |
57.8 |
37.0 |
2.6 |
|
Orange juice (CCM) |
240 |
300 |
36.3 |
109 |
0.8 |
|
Radish |
50 |
14 |
74.4 |
10.4 |
9.2 |
|
Rhubarb |
120 |
174 |
8.54 |
10.1 |
9.5 |
|
Rutabaga |
85 |
36 |
61.4 |
22.1 |
4.4 |
|
Sesame seeds, no hulls |
28 |
37 |
20.8 |
7.7 |
12.2 |
|
Soy milk (tricalcium phosphate) |
240 |
300 |
24.0 |
72.0 |
1.3 |
|
Soy milk (calcium carbonate) |
240 |
300 |
21.1 |
66.3 |
1.0 |
|
Spinach |
85 |
115 |
5.1 |
5.9 |
16.3 |
|
Sweet Potatoes |
164 |
44 |
22.2 |
9.8 |
9.8 |
|
Tofu with Ca |
126 |
258 |
31.0 |
80.0 |
1.2 |
|
Turnip Greens |
72 |
99 |
51.6 |
51.1 |
1.9 |
|
Watercress |
17 |
20 |
67.0 |
13.4 |
7.2 |
|
Yogurt |
240 |
300 |
32.1 |
96.3 |
1.0 |
Notice that the foods high in oxalate like spinach, rhubarb, sweet potatoes, and dried beans are poorly absorbed. But there are still a number of calcium sources outside of milk.
The 2 most common forms of calcium found in supplements are calcium carbonate and calcium citrate. As you can see in the figure below, they differ in the amount of elemental calcium they contain. This shows how much of the molecular weight of the compound is calcium.

Figure 12.221 Percent of calcium supplements that is elemental calcium4
The higher the percent elemental calcium, the greater the amount of calcium you will receive per given weight of that compound, versus a compound that has a lower elemental calcium percentage. Both carbonate and citrate forms are well absorbed, but individuals with low stomach acid absorb citrate better. Also, carbonate is best absorbed when taken with food, while for citrate it is equally well absorbed when taken alone4.
Older research suggested that calcium citrate malate was more bioavailable than other calcium sources. However, a more recent clinical study found no difference in the bioavailability of calcium from calcium citrate malate in orange juice, skim milk, or calcium carbonate supplements5. There is some evidence that suggests that even though bioavailability is the same among these different forms, they might not be equally effective in improving bone measures6.
References & Links
- Weaver CM, Plawecki KL. (1994) Dietary calcium: Adequacy of a vegetarian diet. Am J Clin Nutr 59(5 Suppl): 1238S-1241S.
- Weaver CM, Proulx WR, Heaney R. (1999) Choices for achieving adequate dietary calcium with a vegetarian diet. Am J Clin Nutr 70(3 Suppl): 543S-548S.
- Weaver C. (2009) Closing the gap between calcium intake and requirements. J Am Diet Assoc
109(5): 812-813.
- Martini L, Wood R. (2002) Relative bioavailability of calcium-rich dietary sources in the elderly. Am J Clin Nutr 76(6): 1345-1350.
- Weaver C, Janle E, Martin B, Browne S, Guiden H, et al. (2009) Dairy versus calcium carbonate in promoting peak bone mass and bone maintenance during subsequent calcium deficiency. Journal of Bone and Mineral Research 24(8): 1411-1419.
Calcium Functions
In terms of bone and teeth, calcium is found in bone and referred to as hydroxyapatite (a mineralized form of calcium). There are also a number of non-bone functions of calcium. Calcium is an intracellular signaling molecule. Because of this, intracellular calcium is tightly controlled, primarily stored within organelles.
Non-bone functions include1:
Neurotransmitter release – Neurotransmitter release is stimulated by the opening of voltage- gated Ca2+ channels. This stimulates the synaptic vesicle to fuse with the axon membrane and release the neurotransmitter into the synapse.
Muscle contraction – Calcium is released in muscle cells, where it binds to the protein troponin, changes its shape, and removes the tropomyosin blockade of actin active sites so that contraction can occur2. This can be seen in the following animation and figure (same link).
Required Web LinkMuscle contraction
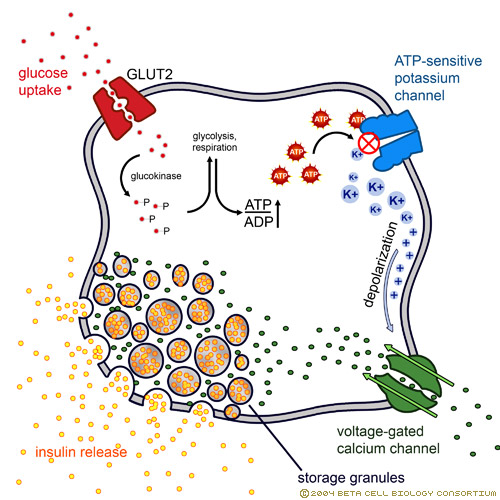
Hormone release – Calcium acts as an intracellular messenger for the release of hormones, such as insulin. The link below shows how in the beta cells of the pancreas, the opening of voltage- gated calcium channels stimulates the insulin granules to fuse with the beta cell membrane to release insulin.
Required Web LinkInsulin release
Blood Clotting – As will be discussed more in the vitamin K section, calcium binding to activated Gla proteins is important in the blood clotting cascade.
Enzyme regulation – The binding of calcium to calcium-binding proteins also regulates the action of a number of enzymes3.
References & Links
1. Byrd-Bredbenner C, Moe G, Beshgetoor D, Berning J. (2009) Wardlaw’s perspectives in nutrition. New York, NY: McGraw-Hill. 2.http://legacy.owensboro.kctcs.edu/GCaplan/anat/Notes/API%20Notes%20J%20%20Muscle% 20Contraction.htm
3. Gropper SS, Smith JL, Groff JL. (2008) Advanced nutrition and human metabolism. Belmont, CA: Wadsworth Publishing.
Links
Muscle contraction – http://legacy.owensboro.kctcs.edu/GCaplan/anat/Notes/API%20Notes%20J%20%20Muscle%2 0Contraction.htm
Insulin release – http://www.dolcera.com/wiki/images/Image11.jpeg
Calcium Deficiency & Toxicity
Because of the large amount of calcium in bones, deficiency is rare1. Hypocalcemia (low serum calcium levels in blood) can result in tetany (involuntary muscle contractions)2. In addition, calcium deficiency in children can lead to rickets, which is a vitamin D deficiency. While not a deficiency, low calcium intake can lead to decreased bone mineral density and the conditions osteopenia and osteoporosis. How these differ from osteomalacia and normal bone is illustrated and described below. There are two different bone components that we will consider to understand what is happening in the bone. Matrix is the scaffolding onto which mineral is deposited. Mineral is at it sounds, the mineral that is deposited on the matrix.
Osteomalacia – Bone mass is normal, but the matrix to mineral ratio is increased, meaning there is less mineral in bone.
Osteopenia – Bone mass is decreased, but the matrix to mineral ratio is not altered from normal bone. This condition is intermediate in between normal and osteoporosis.
Osteoporosis – Bone mass is further decreased from osteopenia, but the matrix to mineral ratio is not altered from normal bone3.
To prevent osteoporosis it is important to build peak bone mass, 90% of which is built in females by age 18 and age 20 in males, but can continue to increase until age 30. After that time, bone mass starts to decrease. For women after menopause, bone mass decreases dramatically because of the decrease in estrogen production, as shown in the link below4.
Required Web LinkBone Mass
Calcium toxicity is rare, occurring in those with hyperparathyroidism or high calcium supplementation levels. Like vitamin D, toxicity can lead to calcification of soft tissues5. In addition, a very high intake of calcium can lead to kidney stone formation.
References & Links
- Shils ME, Shike M, Ross AC, Caballero B, Cousins RJ, editors. (2006) Modern nutrition in health and disease. Baltimore, MD: Lippincott Williams & Wilkins.
- Gropper SS, Smith JL, Groff JL. (2008) Advanced nutrition and human metabolism. Belmont, CA: Wadsworth Publishing.
- Sambrook, P. Bone structure and function in normal and disease states http://v5.books.elsevier.com/bookscat/samples/9780443070150/9780443070150.pdf
- http://www.niams.nih.gov/Health_Info/Bone/Osteoporosis/bone_mass.asp
- Byrd-Bredbenner C, Moe G, Beshgetoor D, Berning J. (2009) Wardlaw’s perspectives in nutrition. New York, NY: McGraw-Hill.
Link
Bone Mass – http://drugline.org/img/term/bone-mass-density-2046_2.gif Bone Mineral Density T-Scores – http://www.orthopaedicsurgeon.com.sg/wp- content/uploads/2011/11/t-scores-large.gif

{kind=link}
{kind=link}
{kind=link}